
Is Your Gut Trying to Tell You Something?
You’ve probably had the experience: a big meal, a stressful week, or just a random Tuesday — and your stomach starts acting up. Bloating, cramping, a sudden urgent need for the bathroom, or the opposite, days of constipation that leave you uncomfortable and frustrated.
For millions of people, this isn’t just an occasional inconvenience. It’s a pattern that disrupts work, social plans, travel, sleep — daily life. And yet, so many people go years without a diagnosis, simply because they’ve normalised the symptoms, or because they’re not sure when something warrants a doctor’s visit.
If any of that sounds familiar, this article is for you. We’re going to break down what IBS actually is, which symptoms should prompt you to seek professional help, and how a gastroenterologist in Pretoria can help you get back to living without planning your day around your digestive system.
IBS affects approximately 10–15% of the global population — making it one of the most common gastrointestinal disorders worldwide.
Source: International Foundation for Gastrointestinal Disorders (IFFGD)
What Is Irritable Bowel Syndrome (IBS)?
Irritable Bowel Syndrome — or IBS — is a chronic condition that affects the large intestine (colon). It’s classified as a functional gastrointestinal disorder, which means the digestive tract looks structurally normal on tests, but doesn’t work the way it should. The gut-brain communication is disrupted, leading to abnormal bowel contractions, increased pain sensitivity, and a range of digestive symptoms.
IBS is not the same as inflammatory bowel disease (IBD), which includes Crohn’s disease and ulcerative colitis. IBD involves visible inflammation and damage to the gut lining — IBS does not. However, the symptoms can overlap significantly, which is one of the key reasons a proper diagnosis matters.
IBS tends to be a long-term condition, but it’s manageable. With the right diagnosis and treatment plan — including dietary adjustments, stress management, and in some cases medication — most people see a significant improvement in their quality of life.
The 4 Types of IBS
IBS is classified into subtypes based on your predominant bowel habit:
| IBS Type | What It Means |
| IBS-D (Diarrhoea-predominant) | More than 25% of stools are loose or watery. Urgency is common. Often triggered by stress, certain foods, or caffeine. |
| IBS-C (Constipation-predominant) | Stools are hard or lumpy more than 25% of the time. Bloating and a feeling of incomplete emptying are frequent complaints. |
| IBS-M (Mixed) | Alternates between diarrhoea and constipation. This is the most common subtype and often the most frustrating to manage. |
| IBS-U (Unclassified) | Symptoms don’t fit neatly into one of the above categories. Still causes significant discomfort and quality-of-life disruption. |
BS Symptoms: What to Look Out For
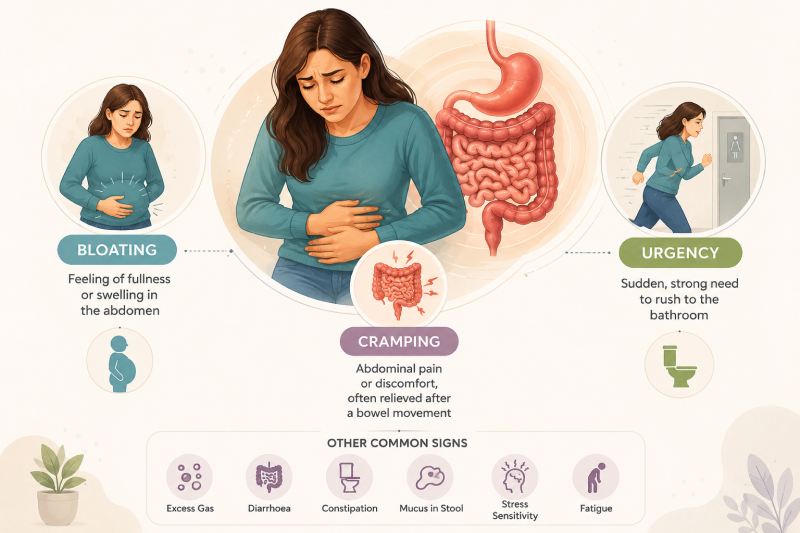
IBS symptoms vary widely from person to person, and they can change over time. The hallmark symptom is recurrent abdominal pain — typically cramping or aching — that is linked to changes in your bowel habits. Here is a full picture of what IBS can feel like:
Core IBS Symptoms
- Abdominal cramping or pain — often relieved (partially or fully) by having a bowel movement
- Bloating and a feeling of fullness or distension — often worse as the day progresses
- Diarrhoea — loose, watery stools, often with urgency and little warning
- Constipation — hard, dry stools that are difficult to pass; a feeling of incomplete emptying
- Alternating diarrhoea and constipation
- Mucus in the stool (without blood)
- Excessive gas and flatulence
Associated Symptoms
IBS doesn’t always stay in the gut. Many patients also experience:
- Fatigue and low energy — often related to disrupted sleep from overnight symptoms
- Nausea, especially after eating
- Anxiety and low mood — the gut-brain connection is well established in IBS
- Backache or pain in the lower back
- Urinary symptoms — needing to urinate more urgently or frequently
- Symptoms that worsen during periods of stress or menstruation (in women)
Source: American Journal of Gastroenterology
IBS vs IBD: Understanding the Crucial Difference
One of the most important distinctions in gastroenterology is the difference between IBS (Irritable Bowel Syndrome) and IBD (Inflammatory Bowel Disease). They sound similar, their symptoms can overlap — but they are fundamentally different conditions requiring very different treatment approaches.
| Feature | IBS | IBD (Crohn’s / Colitis) |
| Gut inflammation | No visible inflammation | Yes — active inflammation present |
| Blood in stool | Rare (not typical) | Common — a key symptom |
| Bowel damage | None | Progressive if untreated |
| Weight loss | Uncommon | Common in active disease |
| Diagnosed by | Symptoms + exclusion of other causes | Colonoscopy, biopsy, imaging |
| Treatment | Diet, lifestyle, medication | Anti-inflammatory drugs, biologics, possible surgery |
| Cancer risk | Not directly increased | Increased with long-standing colitis |
Because symptoms can overlap so significantly, a proper diagnosis from a gastroenterologist in Pretoria is essential. Self-diagnosing IBS and managing it yourself carries the risk of missing a more serious condition like IBD or colorectal cancer. A colonoscopy or other tests may be needed to rule these out.
When Should You See a Gastroenterologist?
Not every stomach ache needs a specialist. But there are specific situations where getting a professional opinion is important — both to confirm an IBS diagnosis and to rule out something more serious.
See a Gastroenterologist If You Have:
- Symptoms that have persisted for more than 3 months
- Abdominal pain that is severe or waking you up at night
- Unexplained weight loss
- Blood in your stool — even a small amount
- Anaemia or unexplained fatigue
- A family history of colorectal cancer, IBD, or coeliac disease
- Symptoms that began after the age of 50
- Rectal bleeding or black/tarry stools
- A significant change in bowel habits that is new and unexplained
⚠️IBS Red Flags — These Always Need Urgent Assessment
- Blood in the stool or rectal bleeding
- Unintentional weight loss (more than 5 kg without trying)
- Symptoms that consistently wake you at night
- Fever alongside abdominal symptoms
- New symptoms starting after age 50
- A family history of bowel cancer or inflammatory bowel disease
These red flag symptoms do not necessarily mean something serious is wrong — but they mean your gut needs a professional evaluation, not a Google search. Book a consultation with Dr. Preetha Thomas if any of these apply to you.
What Causes IBS? The Real Picture
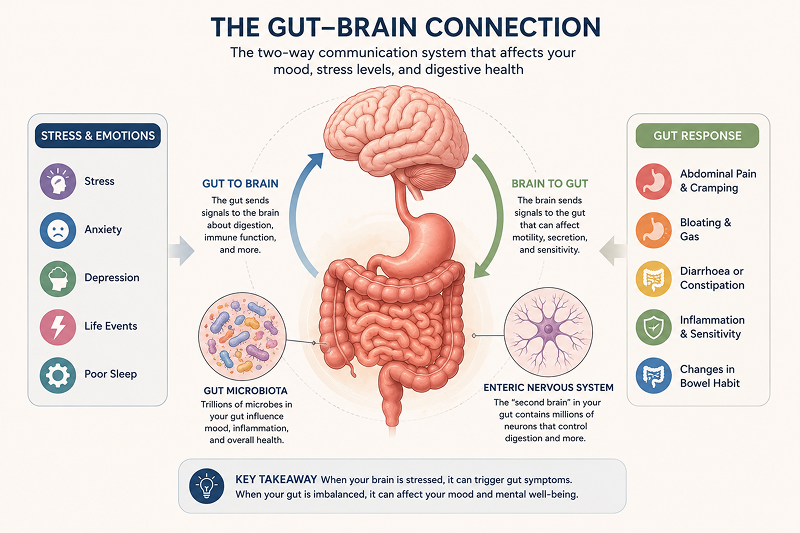
The honest answer is: we don’t fully know. IBS is thought to involve a complex interaction between the gut, the brain, and the nervous system — sometimes called the gut-brain axis. Several factors are known to play a role:
Gut-Brain Dysregulation
In IBS, the nerve signals between the brain and the gut are heightened. The gut becomes hypersensitive — reacting to normal amounts of gas, food, or stress with disproportionate cramping, pain, or urgency. This isn’t psychological weakness; it’s a measurable physiological pattern.
Post-Infectious IBS
A bout of food poisoning or a severe gastroenteritis (stomach flu) can trigger IBS in some people — a condition known as post-infectious IBS. Studies suggest that 5–25% of people develop IBS following a significant gut infection, even after the infection itself has cleared.
Gut Microbiome Imbalance
The trillions of bacteria living in your gut — your microbiome — play a critical role in digestion, immunity, and even mood. In people with IBS, the composition of the gut microbiome is often altered. This can affect gut motility, sensitivity and the production of neurotransmitters like serotonin (95% of which is produced in the gut).
Food Sensitivities and Diet
Certain foods consistently trigger or worsen IBS symptoms for many patients. Common culprits include:
- High-FODMAP foods (fermentable carbohydrates found in onions, garlic, wheat, certain fruits)
- Dairy products — particularly in those with lactose sensitivity
- Caffeine and alcohol
- Fatty or spicy foods
- Artificial sweeteners (especially sorbitol and mannitol)
Stress and Anxiety
Stress doesn’t cause IBS, but it absolutely worsens it. The gut has its own nervous system (the enteric nervous system), which communicates constantly with the brain. Emotional stress, anxiety, or trauma can trigger or amplify IBS flare-ups — which is why psychological support is often part of a holistic IBS treatment plan.
How Is IBS Diagnosed?
There is no single test that diagnoses IBS. It is what’s known as a diagnosis of exclusion — meaning a gastroenterologist rules out other conditions first, and then confirms IBS based on your symptom pattern.
The Rome IV Criteria
Gastroenterologists use the internationally recognised Rome IV criteria to diagnose IBS. Your symptoms must include recurrent abdominal pain at least one day per week over the past three months, associated with two or more of the following:
- Related to defecation (pain improves or worsens with a bowel movement)
- Associated with a change in stool frequency
- Associated with a change in stool consistency or appearance
Tests Your Gastroenterologist May Order
To rule out IBD, coeliac disease, infections, or cancer, your doctor may recommend:
- Blood tests (full blood count, CRP, thyroid function, coeliac antibodies)
- Stool tests (to check for infections, parasites, or markers of inflammation like faecal calprotectin)
- Colonoscopy — to examine the colon and rule out IBD, polyps, or colorectal cancer
- Gastroscopy (upper endoscopy) — to rule out coeliac disease or upper GI causes if you have symptoms like nausea or reflux
- Breath tests — to check for small intestinal bacterial overgrowth (SIBO) or lactose intolerance
💡What to Tell Your Doctor
- Keep a symptom diary for 2–4 weeks before your appointment — note what you eat, stress levels, and symptoms.
- Track the frequency, consistency and urgency of your bowel movements.
- Note what makes symptoms better or worse (specific foods, stress, time of day, menstrual cycle).
- List all medications, supplements, and any recent infections or travel.
IBS Treatment: What Actually Works
The good news about IBS is that it’s very manageable once properly diagnosed. Treatment is personalised — what works for one person may not work for another — but there are well-established strategies with strong evidence.
Dietary Changes
Diet is often the most powerful lever for IBS symptom control. The low-FODMAP diet — developed by researchers at Monash University — has the strongest evidence base. It involves temporarily eliminating foods high in fermentable carbohydrates, then systematically reintroducing them to identify personal triggers.
Other dietary recommendations include:
- Eating smaller, more regular meals rather than large portions
- Reducing caffeine, alcohol, and carbonated drinks
- Increasing soluble fibre (oats, psyllium) for IBS-C; reducing insoluble fibre (bran) if it worsens symptoms
- Staying well hydrated — at least 1.5–2 litres of water daily
Stress Management and Psychological Support
Cognitive behavioural therapy (CBT) and gut-directed hypnotherapy have strong clinical evidence for IBS. Exercise, mindfulness practices, and addressing underlying anxiety or depression can all significantly reduce symptom frequency and severity.
Medication
Depending on your IBS subtype, your gastroenterologist may prescribe:
- Antispasmodics — to reduce bowel cramping and pain
- Laxatives — for IBS-C (constipation-dominant)
- Antidiarrhoeals — for IBS-D (diarrhoea-dominant)
- Low-dose antidepressants — to reduce gut pain sensitivity (not for depression, but gut-brain modulation)
- Peppermint oil capsules — evidence-based for reducing abdominal pain and bloating
- Probiotics — emerging evidence supports specific strains for certain IBS subtypes
Source: Monash University / Clinical Gastroenterology and Hepatology Journal
Related Reading
Digestive symptoms rarely exist in isolation. You may also find these helpful:
- Stomach Pain After Eating: What Could Be Causing Your Discomfort
- GERD vs Acid Reflux: Understanding the Difference — reflux and IBS commonly co-exist
- Colonoscopy in Pretoria: What to Expect Before, During and After — often the first test recommended when IBS symptoms are new
- Meet Dr. Preetha Thomas — specialist gastroenterologist at Mediclinic Kloof, Pretoria
Think You Might Have IBS? Talk to a Gastroenterologist in Pretoria.
You don’t have to manage digestive symptoms alone. Dr. Preetha Thomas offers comprehensive assessment and personalised treatment at Mediclinic Kloof, Erasmuskloof, Pretoria.
Call us: 012 367 4504/5
dr.p.thomas01@gmail.com |Mon–Thu: 9am–5pm · Fri: 9am–1pm
Frequently Asked Questions About IBS
Here are the questions our patients most commonly ask. For personalised advice, contact Dr. Thomas’s practice directly.
Can IBS be cured?
IBS is a chronic condition, which means there is no outright cure — but it is very well manageable. Most patients who receive a proper diagnosis and follow a personalised treatment plan (diet, lifestyle, medication if needed) achieve significant symptom reduction. Many people reach a point where IBS has minimal impact on their daily life. The key is getting an accurate diagnosis so you’re treating the right condition.
How do I know if I have IBS or something more serious?
The symptoms of IBS can overlap with conditions like IBD, coeliac disease, and colorectal cancer — which is exactly why self-diagnosis is risky. Red flags that need urgent investigation include: blood in the stool, unintentional weight loss, symptoms waking you at night, and new symptoms beginning after age 50. If any of these apply, book a consultation with Dr. Preetha Thomas as soon as possible.
Is IBS related to stress?
Stress doesn’t cause IBS, but it is one of the strongest triggers for flare-ups. The gut-brain axis means emotional and psychological stress directly affects gut function. Addressing stress — through exercise, CBT, mindfulness, or psychological support — is a recognised and effective part of IBS management.
What foods should I avoid with IBS?
Common trigger foods include high-FODMAP items (garlic, onions, wheat, certain fruits), dairy, caffeine, alcohol, and fatty or spicy foods. However, triggers are highly individual. A gastroenterologist or registered dietitian can guide you through a structured elimination diet (such as the low-FODMAP protocol) to identify your specific triggers rather than cutting out entire food groups unnecessarily.
Can IBS cause weight loss?
IBS itself does not typically cause significant weight loss. If you are experiencing unexplained weight loss alongside bowel symptoms, this is a red flag that needs urgent assessment — it could suggest IBD, coeliac disease, or another serious condition rather than IBS.
Can children get IBS?
Yes. IBS affects people of all ages, including children and teenagers. In younger patients it is often linked to anxiety, stress, or dietary factors. If your child has recurring abdominal pain and bowel changes, a paediatric gastroenterology referral is appropriate.
Do I need a colonoscopy to diagnose IBS?
Not always — but often yes, particularly if your symptoms are new, you are over 45, or you have any red flag symptoms. A colonoscopy allows the gastroenterologist to rule out IBD, polyps and colorectal cancer, providing the certainty needed to confidently diagnose IBS. It’s a short outpatient procedure performed under sedation at Mediclinic Kloof.
Is IBS hereditary?
There is a moderate genetic component to IBS — you are more likely to have it if a close family member does. However, environmental factors, gut microbiome composition, early life stress, and diet play equally important roles. A family history of bowel problems is worth mentioning to your gastroenterologist.